Pharmacotherapeutic Group: Lipid modifying agents, HMG-CoA-reductase inhibitors.
ATC code: C10AA05.
Pharmacology: Pharmacodynamics: Atorvastatin is a selective, competitive inhibitor of HMG-CoA reductase, the rate-limiting enzyme that converts 3-hydroxy-3-methyl-glutaryl-coenzyme A to mevalonate, a precursor of sterols, including cholesterol. Triglycerides and cholesterol in the liver are incorporated into very low-density lipoprotein (VLDL) and released into the plasma for delivery to peripheral tissues. Low-density lipoprotein (LDL) is formed from VLDL and is catabolised primarily through the receptor with high affinity to LDL (LDL receptors).
Atorvastatin lowers plasma cholesterol and lipoprotein serum concentrations by inhibiting HMG-CoA reductase and subsequently cholesterol biosynthesis in the liver and increases the number of hepatic LDL receptors on the cell surface for enhanced uptake and catabolism of LDL.
Atorvastatin reduces LDL production and the number of LDL particles. Atorvastatin produces a profound and sustained increase in LDL receptor activity coupled with a beneficial change in the quality of circulating LDL particles. Atorvastatin is effective in reducing LDL-C in patients with homozygous familial hypercholesterolaemia, a population that has not usually responded to lipid-lowering medicinal products.
Atorvastatin has been shown to reduce concentrations of total-C (30%-46%), LDL-C (41%-61%), apolipoprotein B (34%-50%), and triglycerides (14% - 33%) while producing variable increases in HDL-C and apolipoprotein A1 in a dose response study. These results are consistent in patients with heterozygous familial hypercholesterolaemia, nonfamilial forms of hypercholesterolaemia, and mixed hyperlipidaemia, including patients with noninsulindependent diabetes mellitus.
Reductions in total-C, LDL-C, and apolipoprotein B have been proven to reduce risk for cardiovascular events and cardiovascular mortality
Homozygous familial hypercholesterolaemia: In a multicenter 8 week open-label compassionate-use study with an optional extension phase of variable length, 335 patients were enrolled, 89 of which were identified as homozygous familial hypercholesterolaemia patients. From these 89 patients, the mean percent reduction in LDL-C was approximately 20%. Atorvastatin was administered at doses up to 80 mg/day.
Atherosclerosis: In the Reversing Atherosclerosis with Aggressive Lipid- Lowering Study (REVERSAL), the effect of intensive lipid lowering with atorvastatin 80 mg and standard degree of lipid lowering with pravastatin 40 mg on coronary atherosclerosis was assessed by intravascular ultrasound (IVUS), during angiography, in patients with coronary heart disease. In this randomised, double- blind, multicenter, controlled clinical trial, IVUS was performed at baseline and at 18 months in 502 patients. In the atorvastatin group (n=253), there was no progression of atherosclerosis.
The median percent change, from baseline, in total atheroma volume (the primary study criteria) was -0.4% (p=0.98) in the atorvastatin group and +2.7% (p=0.001) in the pravastatin group (n=249). When compared to pravastatin the effects of atorvastatin were statistically significant (p=0.02). The effect of intensive lipid lowering on cardiovascular endpoints (e. g. need for revascularisation, non fatal myocardial infarction, coronary death) was not investigated in this study.
In the atorvastatin group, LDL-C was reduced to a mean of 2.04 mmol/L ± 0.8 (78.9 mg/dl ± 30) from baseline 3.89 mmol/L ± 0.7 (150 mg/dl ± 28) and in the pravastatin group, LDL-C was reduced to a mean of 2.85 mmol/L ± 0.7 (110 mg/dl ± 26) from baseline 3.89 mmol/L ± 0.7 (150 mg/dl ± 26) (p<0.0001). Atorvastatin also significantly reduced mean TC by 34.1% (pravastatin: -18.4%, p<0.0001), mean TG levels by 20% (pravastatin: -6.8%, p<0.0009), and mean apolipoprotein B by 39.1% (pravastatin: -22.0%, p<0.0001). Atorvastatin increased mean HDL-C by 2.9% (pravastatin: +5.6%, p=NS). There was a 36.4% mean reduction in CRP in the atorvastatin group compared to a 5.2% reduction in the pravastatin group (p<0.0001).
Study results were obtained with the 80 mg dose strength. Therefore, they cannot be extrapolated to the lower dose strengths.
The safety and tolerability profiles of the two treatment groups were comparable. The effect of intensive lipid lowering on major cardiovascular endpoints was not investigated in this study. Therefore, the clinical significance of these imaging results with regard to the primary and secondary prevention of cardiovascular events is unknown.
Acute coronary syndrome: In the MIRACL study, atorvastatin 80 mg has been evaluated in 3,086 patients (atorvastatin n=1,538; placebo n=1,548) with an acute coronary syndrome (non Q-wave MI or unstable angina). Treatment was initiated during the acute phase after hospital admission and lasted for a period of 16 weeks. Treatment with atorvastatin 80 mg/day increased the time to occurrence of the combined primary endpoint, defined as death from any cause, nonfatal MI, resuscitated cardiac arrest, or angina pectoris with evidence of myocardial ischaemia requiring hospitalization, indicating a risk reduction by 16% (p=0.048). This was mainly due to a 26% reduction in re-hospitalisation for angina pectoris with evidence of myocardial ischaemia (p=0.018). The other secondary endpoints did not reach statistical significance on their own (overall: Placebo: 22.2%, Atorvastatin: 22.4%).
The safety profile of atorvastatin in the MIRACL study was consistent with what is described in Adverse Reactions.
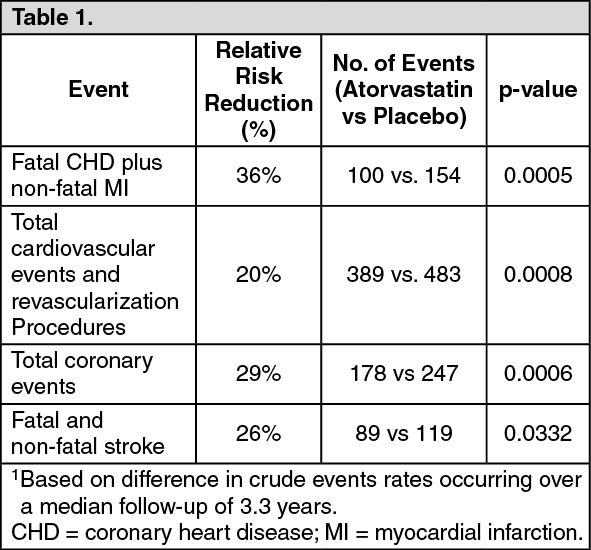
Prevention of cardiovascular disease: The effect of atorvastatin on fatal and non-fatal coronary heart disease was assessed in a randomized, double-blind, placebocontrolled study, the Anglo-Scandinavian Cardiac Outcomes Trial Lipid Lowering Arm (ASCOT-LLA). Patients were hypertensive, 40-79 years of age, with no previous myocardial infarction or treatment for angina, and with TC levels ≤6.5 mmol/L (251 mg/dl). All patients had at least 3 of the pre-defined cardiovascular risk factors: male gender, age ≥55 years, smoking, diabetes, history of CHD in a first-degree relative, TC:HDL-C >6, peripheral vascular disease, left ventricular hypertrophy, prior cerebrovascular event, specific ECG abnormality, proteinuria/albuminuria. Not all included patients were estimated to have a high risk for a first cardiovascular event. Patients were treated with anti-hypertensive therapy (either amlodipine or atenolol-based regimen) and either atorvastatin 10 mg daily (n=5,168) or placebo (n=5,137).
The relative risk reduction effect of atorvastatin was as follows: (see Table 1).
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Total mortality and cardiovascular mortality were not significantly reduced (185 vs. 212 events, p=0.17 and 74 vs. 82 events, p=0.51). In the subgroup analyses by gender (81% males, 19% females), a beneficial effect of atorvastatin was seen in males but could not be established in females possibly due to the low event rate in the female subgroup. Overall and cardiovascular mortality were numerically higher in the female patients (38 vs. 30 and 17 vs. 12), but this was not statistically significant. There was significant treatment interaction by antihypertensive baseline therapy. The primary endpoint (fatal CHD plus non-fatal MI) was significantly reduced by atorvastatin in patients treated with amlodipine (HR 0.47 (0.32-0.69), p=0.00008), but not in those treated with atenolol (HR 0.83 (0.59-1.17), p=0.287).
The effect of atorvastatin on fatal and non-fatal cardiovascular disease was also assessed in a randomized, double- blind,multicenter, placebo-controlled trial, the Collaborative Atorvastatin Diabetes Study (CARDS) in patients with type 2 diabetes, 40-75 years of age, without prior history of cardiovascular disease, and with LDL-C ≤4.14 mmol/L (160 mg/dl) and TG ≤6.78 mmol/L(600 mg/dl). All patients had at least 1 of the following risk factors: hypertension, current smoking, retinopathy, microalbuminuria or macroalbuminuria.
Patients were treated with either atorvastatin 10 mg daily (n=1,428) or placebo (n=1,410) for a median follow-up of 3.9 years.
The relative risk reduction effect of atorvastatin was as follows: (see Table 2).
Click on icon to see table/diagram/image
There was no evidence of a difference in the treatment effect by patient's gender, age, or baseline LDL-C level. A favourable trend was observed regarding the mortality rate (82 deaths in the placebo group vs. 61 deaths in the atorvastatin group, p=0.0592).
Recurrent stroke: In the Stroke Prevention by Aggressive Reduction in Cholesterol Levels (SPARCL) study, the effect of atorvastatin 80 mg daily or placebo on stroke was evaluated in 4731 patients who had a stroke or transient ischemic attack (TIA) within the preceding 6 months and no history of coronary heart disease (CHD). Patients were 60% male, 21-92 years of age (average age 63 years), and had an average baseline LDL of 133 mg/dl (3.4 mmol/l). The mean LDL-C was 73 mg/dl (1.9 mmol/l) during treatment with atorvastatin and 129 mg/dl (3.3 mmol/l) during treatment with placebo. Median follow-up was 4.9 years.
Atorvastatin 80 mg reduced the risk of the primary endpoint of fatal or non-fatal stroke by 15% (HR 0.85; 95% CI, 0.72-1.00; p=0.05 or 0.84; 95% CI, 0.71-0.99; p=0.03 after adjustment for baseline factors) compared to placebo. All cause mortality was 9.1% (216/2365) for atorvastatin versus 8.9% (211/2366) for placebo.
In a post-hoc analysis, atorvastatin 80 mg reduced the incidence of ischemic stroke (218/2365, 9.2% vs. 274/2366, 11.6%, p=0.01) and increased the incidence of hemorrhagic stroke (55/2365, 2.3% vs. 33/2366, 1.4%, p=0.02) compared to placebo.
The risk of hemorrhagic stroke was increased in patients who entered the study with prior hemorrhagic stroke (7/45 for atorvastatin versus 2/48 for placebo; HR 4.06; 95% CI, 0.84- 19.57), and the risk of ischemic stroke was similar between groups (3/45 for atorvastatin versus 2/48 for placebo; HR 1.64; 95% CI, 0.27-9.82).
The risk of hemorrhagic stroke was increased in patients who entered the study with prior lacunar infarct (20/708 for atorvastatin versus 4/701 for placebo; HR 4.99; 95% CI, 1.71- 14.61), but the risk of ischemic stroke was also decreased in these patients (79/708 for atorvastatin versus 102/701 for placebo; HR 0.76; 95% CI, 0.57-1.02). It is possible that the net risk of stroke is increased in patients with prior lacunar infarct who receive atorvastatin 80 mg/day.
All cause mortality was 15.6% (7/45) for atorvastatin versus 10.4% (5/48) in the subgroup of patients with prior hemorrhagic stroke. All cause mortality was 10.9% (77/708) for atorvastatin versus 9.1% (64/701) for placebo in the subgroup of patients with prior lacunar infarct.
Paediatric Population: Heterozygous Familial Hypercholesterolaemia in Paediatric Patients aged 6-17 years old: An 8-week, open-label study to evaluate pharmacokinetics, pharmacodynamics, and safety and tolerability of atorvastatin was conducted in children and adolescents with genetically confirmed heterozygous familial hypercholesterolemia and baseline LDLC ≥4 mmol/L. A total of 39 children and adolescents, 6 to 17 years of age, were enrolled. Cohort A included 15 children, 6 to 12 years of age and at Tanner Stage 1. Cohort B included 24 children, 10 to 17 years of age and at Tanner Stage ≥2.
The initial dose of atorvastatin was 5 mg daily of a chewable tablet in Cohort A and 10 mg daily of a tablet formulation in Cohort B. The atorvastatin dose was permitted to be doubled if a subject had not attained target LDL-C of <3.35 mmol/L at Week 4 and if atorvastatin was well tolerated.
Mean values for LDL-C, TC, VLDL-C, and Apo B decreased by Week 2 among all subjects. For subjects whose dose was doubled, additional decreases were observed as early as 2 weeks, at the first assessment, after dose escalation. The mean percent decreases in lipid parameters were similar for both cohorts, regardless of whether subjects remained at their initial dose or doubled their initial dose. At Week 8, on average, the percent change from baseline in LDL-C and TC was approximately 40% and 30%, respectively, over the range of exposures.
Heterozygous Familial Hypercholesterolaemia in Paediatric Patients aged 10-17 years old: In a double-blind, placebo controlled study followed by an open-label phase, 187 boys and postmenarchal girls 10-17 years of age (mean age 14.1 years) with heterozygous familial hypercholesterolaemia (FH) or severe hypercholesterolaemia were randomised to atorvastatin (n=140) or placebo (n=47) for 26 weeks and then all received atorvastatin for 26 weeks. The dosage of atorvastatin (once daily) was 10 mg for the first 4 weeks and uptitrated to 20 mg if the LDL-C level was >3.36 mmol/l. Atorvastatin significantly decreased plasma levels of total-C, LDL-C, triglycerides, and apolipoprotein B during the 26 week double-blind phase. The mean achieved LDL-C value was 3.38 mmol/l (range: 1.81-6.26 mmol/l) in the atorvastatin group compared to 5.91 mmol/l (range: 3.93-9.96 mmol/l) in the placebo group during the 26-week double-blind phase.
An additional paediatric study of atorvastatin versus colestipol in patients with hypercholesterolaemia aged 10-18 years demonstrated that atorvastatin (N=25) caused a significant reduction in LDL-C at week 26 (p<0.05) compared with colestipol (N=31).
A compassionate use study in patients with severe hypercholesterolaemia (including homozygous hypercholesterolaemia) included 46 paediatric patients treated with atorvastatin titrated according to response (some subjects received 80 mg atorvastatin per day). The study lasted 3 years: LDL-cholesterol was lowered by 36%.
The long-term efficacy of atorvastatin therapy in childhood to reduce morbidity and mortality in adulthood has not been established.
Pharmacokinetics: Absorption: Atorvastatin is rapidly absorbed after oral administration; maximum plasma concentrations (C
max) occur within 1 to 2 hours. Extent of absorption increases in proportion to atorvastatin dose. After oral administration, atorvastatin film-coated tablets are 95% to 99% bioavailability compared to the oral solution. The absolute bioavailability of atorvastatin (parent medicinal product) is approximately 12% and the systemic availability of HMG-CoA reductase inhibitory activity is approximately 30%. The low systemic availability is attributed to presystemic clearance in gastrointestinal mucosa and/or hepatic first-pass metabolism.
Distribution: Mean volume of distribution of atorvastatin is approximately 381 liters. Atorvastatin is ≥ 98% bound to plasma proteins.
Biotransformation: Atorvastatin is metabolized by cytochrome P450 3A4 to ortho- and parahydroxylated derivatives and various beta-oxidation products. Apart from other pathways these products are further metabolized via glucuronidation.
In vitro inhibition of HMG-CoA reductase by ortho- and parahydroxylated metabolites is equivalent to that of atorvastatin. Approximately 70% of circulating inhibitory activity for HMG-CoA reductase is attributed to active metabolites.
Elimination: Atorvastatin is eliminated primarily in bile following hepatic and/or extrahepatic metabolism; However, atorvastatin does not appear to undergo significant enterohepatic recirculation. Mean plasma elimination half-life of atorvastatin in humans is approximately 14 hours. The half-life of inhibitory activity for HMG-CoA reductase is approximately 20 to 30 hours due to the contribution of active metabolites.
Special populations: Elderly: Plasma concentrations of atorvastatin and its active metabolites are higher in healthy elderly subjects than in young adults while the lipid effects were comparable to those seen in younger patient populations.
Paediatric: In an open-label, 8-week study, Tanner Stage 1 (N=15) and Tanner Stage ≥2 (N=24) paediatric patients (ages 6-17 years) with heterozygous familial hypercholesterolemia and baseline LDL-C ≥4 mmol/l were treated with 5 or 10 mg of chewable or 10 or 20 mg of film-coated atorvastatin tablets once daily, respectively. Body weight was the only significant covariate in atorvastatin population PK model. Apparent oral clearance of atorvastatin in paediatric subjects appeared similar to adults when scaled allometrically by body weight. Consistent decreases in LDL-C and TC were observed over the range of atorvastatin and ohydroxyatorvastatin exposures.
Gender: Concentrations of atorvastatin and its active metabolites in women differ from those in men (Women: approximately 20% higher for C
max and appox. 10% lower for AUC); These differences were of no clinically significance, resulting in on clinically significant differences in lipid effects among men and women.
Patients with renal impairment: Renal disease has no influence on the plasma concentrations or lipid effects of atorvastatin and its active metabolites.
Hemodialysis: While studies have not been conducted in patients with end-stage renal disease, hemodialysis is not expected to significantly enhance clearance of atorvastatin since the medicinal product is extensively bound to plasma proteins.
Patients with hepatic impairment: Plasma concentrations of atorvastatin and its active metabolites are markedly increased (approx. 16-fold in C
max and approx. 11-fold in AUC) in patients with chronic alcoholic liver disease (Child-Pugh B).
SLOC1B1 polymorphism: Hepatic uptake of all HMG-CoA reductase inhibitors including atorvastatin, involves the OATP1B1 transporter. In patients with SLCO1B1 polymorphism there is a risk of increased exposure of atorvastatin, which may lead to an increased risk of rhabdomyolysis (see Precautions). Polymorphism in the gene encoding OATP1B1 (SLCO1B1 c.521CC) is associated with a 2.4-fold higher atorvastatin exposure (AUC) than in individuals without this genotype variant (c.521TT). A genetically impaired hepatic uptake of atorvastatin is also possible in these patients. Possible consequences for the efficacy are unknown.
Toxicology: Preclinical safety data: Atorvastatin was negative for mutagenic and clastogenic potential in a battery of 4 in vitro tests and 1 in vivo assay. Atorvastatin was not found to be carcinogenic in rats, but high doses in mice (resulting in 6-11 fold the AUC0-24h reached in humans at the highest recommended dose) showed hepatocellular adenomas in males and hepatocellular carcinomas in females.
There is evidence from animal experimental studies that HMG-CoA reductase inhibitors may affect the development of embryos or fetuses. In rats, rabbits and dogs atorvastatin had no effect on fertility and was not teratogenic, however, at maternally toxic doses fetal toxicity was observed in rats and rabbits. The development of the rat offspring was delayed and post-natal survival reduced during exposure of the dams to high doses of atorvastatin. In rats, there is evidence of placental transfer. In rats, plasma concentrations of atorvastatin are similar to those in milk.
It is not known whether atorvastatin or its metabolites are excreted in human milk.


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image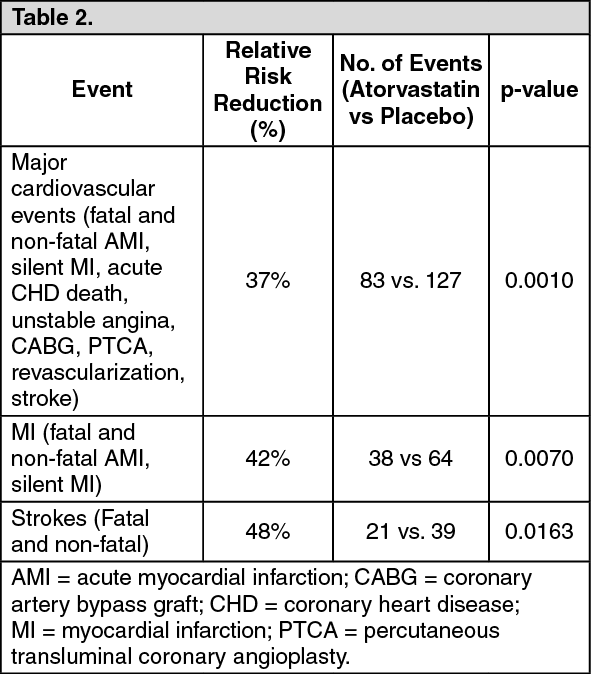 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image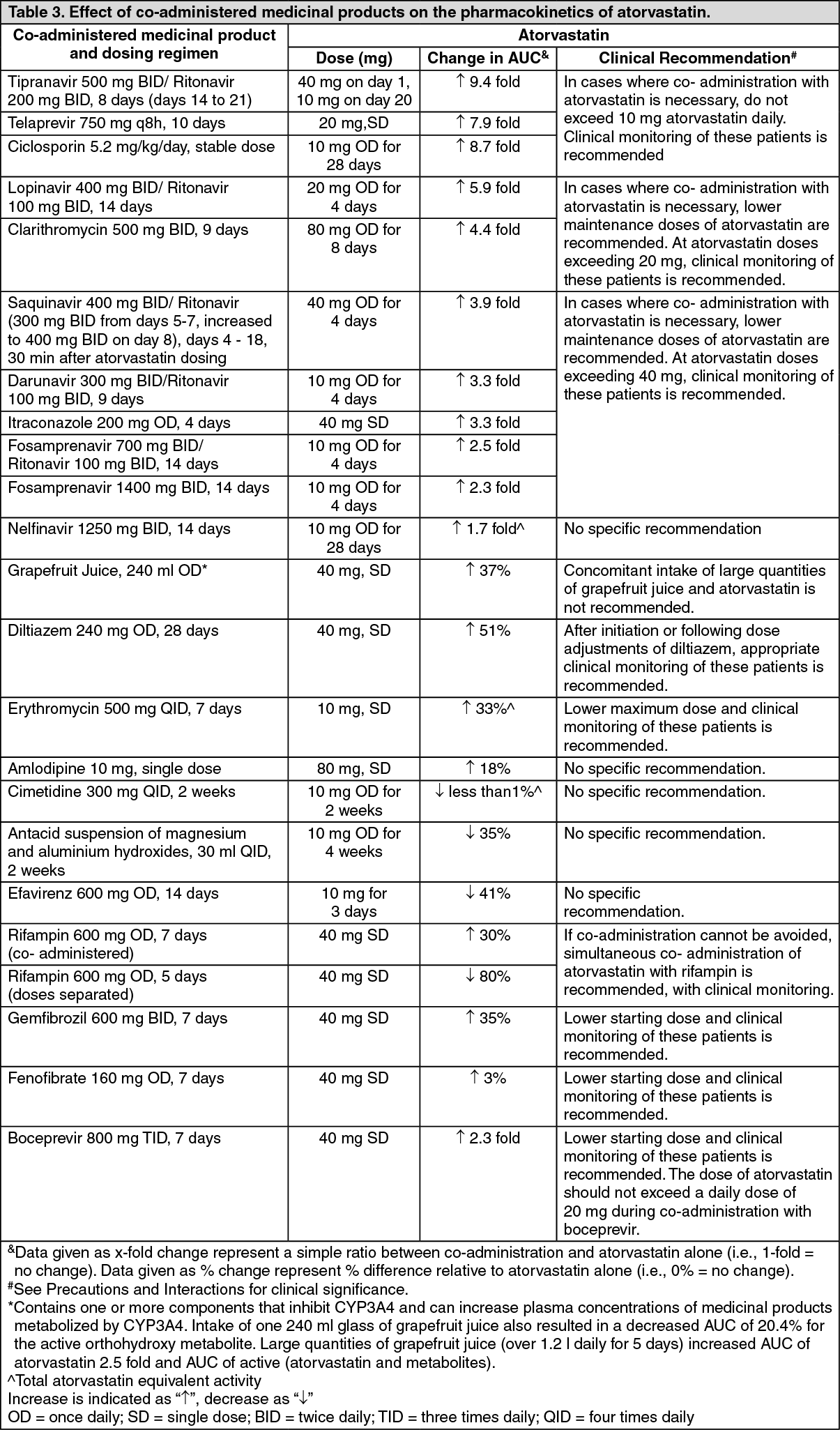 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image



 Sign Out
Sign Out
